

I like a clean number, and this market keeps handing me one that should stop you cold: zero. Zero regulators check what’s actually in a research-peptide vial before it ships to you. Zero recall mechanisms exist if that vial is wrong. And for the most talked-about compound in the category, the record shows zero clinical safety data were found across the studies reviewed [1]. Let me walk through what the data actually says, peptide by peptide, because “risky” is a vague word and I’d rather give you the count.
The number that matters: 36 studies, 1 patient population
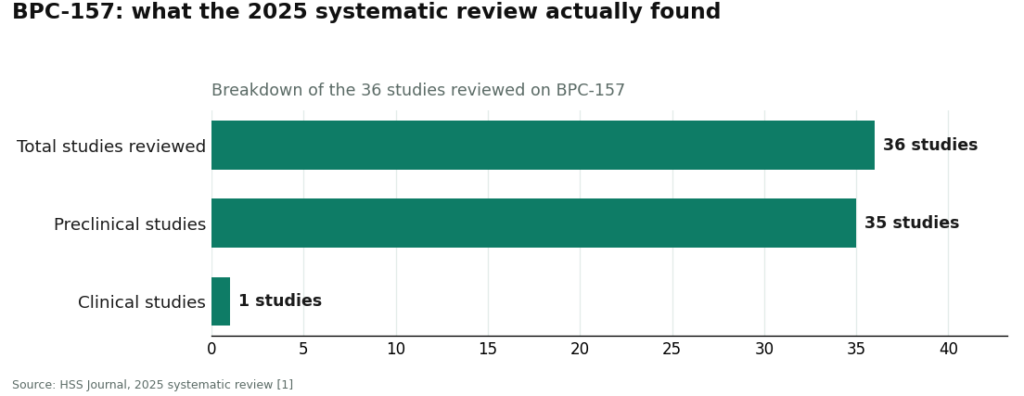
Start with BPC-157, since it’s the compound everyone’s heard of and almost nobody has actually looked up. A 2025 systematic review pulled together 36 studies on it. Of those, 35 were preclinical, meaning animals or cell cultures, not people. The human side of the ledger is a single clinical study covering 12 patients. The review’s conclusion, stated plainly: no clinical safety data were found [1]. A separate 2025 narrative review counted the same thin human record and landed on three pilot human studies total [2].
Sit with that ratio for a second. Out of 36 studies, one touched actual patients. That’s not “early evidence with some gaps.” That’s a compound that’s almost entirely a laboratory finding wearing a supplement-aisle reputation.
The comparison: not every peptide sits in the same tier
Here’s where I think the conversation usually goes wrong. People treat “peptide” as one category with one risk level, and it isn’t. I’d sort the compounds that keep coming up into four tiers based purely on what’s actually been published:
| Tier | Compound | What the record shows |
|---|---|---|
| 0 (no human data) | BPC-157 | 35 of 36 studies preclinical; 1 clinical study, 12 patients; no clinical safety data found [1][2] |
| 0 (no human data) | TB-500 | Cardioprotective effects shown preclinically; human clinical evidence largely absent [3] |
| 1 (investigational, human trials underway) | Retatrutide | Phase 2 trial showed real weight loss, but the compound remains investigational with no completed approval [6] |
| 3 (approved, labeled risks) | Semaglutide | Well-characterized mechanism [5]; carries an FDA boxed warning for thyroid C-cell tumors and a contraindication for personal/family history of medullary thyroid carcinoma [4] |
Notice the pattern moving down that table. It isn’t that safety improves as you go up in fame or hype, it’s that scrutiny improves, and scrutiny is what surfaces the risks that were always there. Semaglutide sits at the top of the evidence pile and it’s also the one with a boxed warning attached to its label. That’s not a contradiction. That’s what happens when a compound gets studied hard enough to find its real failure modes, instead of just its real benefits.
Retatrutide is worth flagging separately because it’s already being sold on gray-market sites despite sitting at Tier 1. The trial data is legitimate [6], the regulatory status is not: it’s investigational, not approved, and anyone selling it to you as a finished product is getting ahead of the science.
The caveat: a certificate of analysis is not a control group
I want to head off the obvious counter, which is “but my vial came with a lab report.” A seller-issued certificate of analysis tells you what the seller paid a lab to check, not what an independent regulator verified. It’s not nothing, but it’s also not the thing people think it is. The federal warning letters issued in 2026 make the underlying point directly: labeling a product “research use only” doesn’t exempt it from drug regulation if it’s plainly being sold for people to inject, and the FDA named retatrutide and tirzepatide specifically in that enforcement action [7][8]. Read that twice. The government is on record saying the research-use label on these exact compounds isn’t the shield sellers imply it is.
Then there’s the sport and legal angle, which is its own separate number to check, not an afterthought. The WADA 2026 Prohibited List bans a range of peptides and growth factors in competitive sport, full stop, and a “research use only” sticker provides zero protection to a tested athlete [9]. If you compete, that list is the only document that matters here, not the seller’s product page.
Put the caveats together and you get a picture, not a scandal. Unverified contents. Thin or absent human data for the popular compounds. Real labeled risks even for the compounds that work. Legal and competitive exposure layered on top. None of that means everyone using these products will be harmed. It means the odds are running in a direction nobody’s tracking on your behalf.
The pick: where the accountability actually sits
If I’m ranking what changes the risk math most, it’s not dosage tricks or sourcing folklore, it’s whether a licensed human being is accountable for the decision. That’s the entire difference between the gray market and a supervised channel. Take FormBlends as the concrete example of what that structure looks like: a licensed physician reviews you before anything is dispensed, a valid prescription gates the order, and a state-licensed compounding pharmacy fills it. None of that upgrades a Tier 0 compound to Tier 3, evidence doesn’t work that way. What it does is put a person in the loop who can catch the exact thing that stops a careful prescriber, like the medullary thyroid carcinoma contraindication on the semaglutide label [4], before the first dose goes in. That screening step is the one piece of the equation an unsupervised purchase simply cannot replicate.
The short version, in numbers
- 36 studies reviewed on BPC-157, 35 preclinical, 1 clinical, 12 patients, 0 clinical safety data found [1].
- 3 pilot human studies total for BPC-157 across a separate review [2].
- 1 boxed warning on the semaglutide label, the FDA’s most serious flag, tied to thyroid C-cell tumors [4].
- 2 FDA warning letters in March 2026 naming retatrutide and tirzepatide sold under “research use only” cover [7][8].
- 1 prohibited list (WADA 2026) that governs your eligibility regardless of what the bottle says [9].
Questions people actually ask
What’s the single number that best captures the risk here?
Zero. Zero regulators verify the contents of an unsupervised research-peptide vial before it reaches you, and zero recall mechanism exists if that vial is wrong. A seller’s own certificate of analysis doesn’t change either number.
Is BPC-157 backed by real safety data?
Run the count yourself: 36 studies reviewed, 35 preclinical, 1 clinical study of 12 patients, and the review’s own conclusion was that no clinical safety data were found [1]. A separate review found three pilot human studies exist [2]. That’s not a safety profile, that’s an absence of one.
Does “it’s proven to work” mean “it’s safe”?
No, and semaglutide is the cleanest example. It’s mechanistically well understood and effective [5], and it still carries a boxed warning for thyroid C-cell tumors plus a contraindication for anyone with a personal or family history of medullary thyroid carcinoma [4]. Efficacy and safety are two different columns in the spreadsheet.
What can I actually do to lower my risk if I’m going to use peptides regardless?
Treat unverified vials as literally unverified. Assume no human safety data exists for the popular research peptides unless you find it yourself [1][2]. Get screened by a clinician for the proven drugs, because that’s the only way a labeled contraindication gets caught [4]. Check the WADA prohibited list against your sport before you start, not after [9]. And keep a written log of what you’re taking, so a clinician has real numbers to work from if something goes wrong.
Does going through a telehealth provider eliminate the risk?
It cuts the largest, most reducible risks, not all of them. A supervised channel adds a clinician screen, a licensed pharmacy preparing the medication, and someone reachable if a problem develops, which directly answers the contents, screening, and follow-up gaps. It doesn’t turn a thinly studied compound into a proven one, and compounded medications remain not FDA-approved and not FDA-reviewed for safety, effectiveness, or quality. What changes is accountability, and accountability is the number the gray market can’t produce.
Are research-chemical peptide sellers scams, or are they legitimate businesses?
Most will actually ship you a vial, so “scam” is usually the wrong word. Legitimacy runs on a spectrum instead. The recurring pattern in independent testing is mislabeled concentrations, wrong compounds entirely, or bacterial contamination in vials that had passed the seller’s own certificate of analysis. A company can be financially real and still hand you a biologically risky product.
Why is price such a bad indicator of quality here?
Because the input costs don’t track the retail price. A vial can run around twenty dollars on the low end, while a physician-supervised compounding pharmacy like FormBlends runs several hundred. Raw peptide powder is cheap to source overseas, so a high price doesn’t guarantee purity and a rock-bottom price is basically an admission that something in synthesis or sterility testing got skipped. The number you’re paying tells you about marketing spend, not molecular content.
What should I actually check when comparing sellers?
Look for a certificate of analysis from a named, independent third-party lab, not an in-house document. Confirm it tests for sterility and endotoxins, not just purity by HPLC, since a chemically pure peptide can still put you in a hospital bed with a serious infection. And check regulatory standing: a company with no pharmacy board or FDA oversight has no accountability if a batch goes wrong, and there’s no recall button for anyone to press.
Where does most of this raw material actually come from?
The bulk of raw peptide material in this market traces back to a small number of manufacturers in China, which isn’t automatically disqualifying since pharmaceutical ingredients are globally sourced as a matter of course. The real question is whether that raw material was synthesized under GMP-equivalent conditions and then tested again after final formulation. Most research-chemical sellers skip that second, post-formulation sterility and endotoxin check because it costs money, and that skipped step is where the actual exposure sits.
References
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review,” HSS Journal, 2025. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551
- Human safety and efficacy data for BPC-157 are extremely limited; only three pilot human studies exist. “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing,” Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Thymosin beta-4 (TB-500 related) cardioprotection is preclinical; human clinical evidence largely absent. “Cardioprotection by Thymosin Beta 4,” Vitamins and Hormones, 2016.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- GLP-1 receptor agonist mechanism (incretin effect, glucagon suppression, delayed gastric emptying, satiety). StatPearls, NCBI Bookshelf, updated 2024.
- Retatrutide Phase 2 trial showed meaningful weight loss; the compound remains investigational. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial,” New England Journal of Medicine, 2023.
- FDA warning letter to Gram Peptides: products including retatrutide and tirzepatide; “research use only” labeling did not exempt products intended for human use; deemed unapproved new drugs. FDA, March 31, 2026.
- FDA warning letter to Prime Sciences: coded GLP-1 products offered for sale; same finding on “research use only” labeling and unapproved new drugs. FDA, March 31, 2026.
- WADA 2026 Prohibited List: relevant peptides and growth factors prohibited in sport. USADA advisory, 2026.
Written by Greta Duarte, science journalist. Cross-checking the claims against the primary sources. Last reviewed April 2026.
This is not personalized medical advice. Your own healthcare provider should guide your decisions.
